|
|
Alveolar Sarcoid
General Considerations
- Least common manifestation of sarcoid in the lungs (2%)
- Several large airspace “masses” frequently with air bronchograms
- Occurs when granulomas become confluent and compress airspaces
Clinical Findings
- May have an abrupt onset and may change rapidly
Imaging Findings
- Bilateral, multifocal, ill-defined nodules mimicking airspace disease
- May be peripheral in lung, like pulmonary infiltrates with eosinophilia
- “Masses” with air bronchograms
- May very rarely have cavitation
- Gallium 67 will be taken up in sarcoid and may show extranodal sites of involvement, but is not specific
Differential Diagnosis
- Alveolar cell carcinoma
- Lymphoma
- Alveolar proteinosis
- Multifocal pneumonia
Treatment
- Alveolar sarcoid tends to improve with or without steroids
Complications
- High risk for spontaneous pneumothorax
Prognosis
- The “airspace” component of pulmonary sarcoid invariably disappears
- Reticulonodular disease may remain


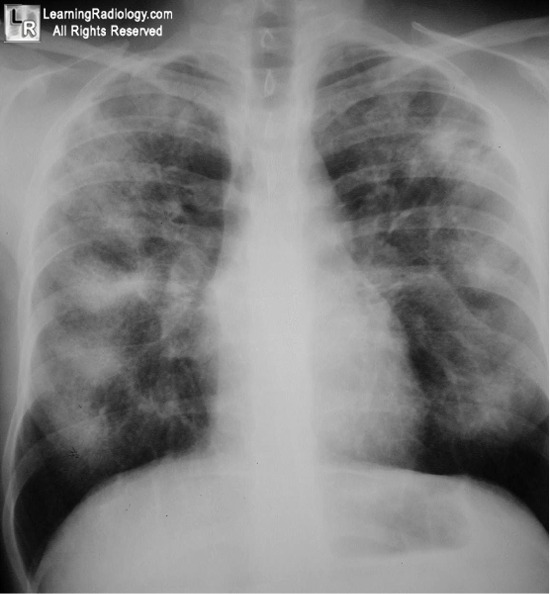
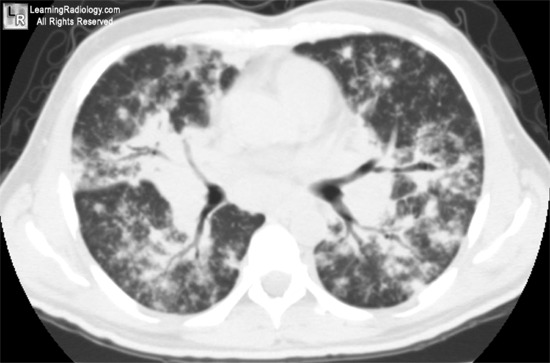
Alveolar Sarcoid. Frontal chest radiograph at left demonstrates multiple, scattered mass-like densities with irregular margins. The disease affects primarily the periphery of the lungs. A CT scan of another patient with alveolar sarcoid (right) shows multiple patchy densities with air bronchograms (black arrows).
For more information, click on the link if you see this icon 
For this same photo without the annotations, click here and here
|
|
|

{kind=link}
{kind=link}